WOur brain is not a black box any more - in this chapter, we will take a closer look at processes of
the brain concerned with language comprehension. Dealing with natural language understanding, we
distinguish between the neuroscientific and the psycholinguistic approach. As text understanding
spreads through the broad field of cognitive psychology, linguistics, and neurosciences, our main focus
will lay on the intersection of two latter, which is known as neurolinguistics.
Different brain areas need to be examined in order to find out how words and sentences are being
processed. Since there are only limited possibilities of acquiring knowledge about brain states under
natural conditions, we are restricted to draw conclusions from certain brain lesions to the functions of
corresponding brain areas.
Hence, much research is done on those brain lesions that cause speech processing deficiencies
(aphasiae). One of the most famous examples is Broca's aphasia, which is caused by a lesion of the
frontal brain region. A typical symptom is telegraphese speech without grammar, while speech
understanding is mainly unaffected. In contrast, persons suffering from Wernickes aphasia, an also
well-known disruption of a more posterior brain region, speak very fluently, using neologisms
(building of new words not belonging to the language) as well as phonematic and semantic
paraphrasiae (substitution of a phoneme of the word by another one) but have a heavily impaired
language understanding.
To examine these brain lesions, techniques for brain imaging and ERP-measurement have been
established during the last 40 years. These devices contribute to the acquired data more and more
adequate: The possibly best established brain imaging technique is the so called PET (positron
emission tomography) scan, which was introduced in the 1970s. It maps the bloodflow in brain areas of
interest onto colored “brain-activity-pictures” by measuring the activity of a radioactive tracer injected
into the living person’s blood. An analogous principle we find at fMRI-scans (functional magnetic
resonance imaging). This (newer) method of brain imaging works without the use of radioactivity and
is therefore non-intrusive and less injurious. Therefore it can be applied on a patient repetitivley as it
might be needed for follow up studies. This technique works with the blood's substances responding to
magnetic fields. EEG (Electroencephalography) records the electrical activity in the brain by placing
electrodes on the scalp. Unlike PET and fMRI, it does not produce images, but istead waves which
precisely show the size of activity for a given stimuli.
Scientific studies on these phenomena are generally divided into research on auditory and visual
language comprehension; we will discuss both and have a glance at their differences and similarities.
And not to forget is that it is not enough to examine English: To understand language processing in
general, we have to look at non-Indoeuropean and other language systems like sign language also.
Today there are several theories about the roles of different brain domains in language
understanding. For there is still a lot to do in this exciting field of current research.
94 | Cognitive Psychology and Neuroscience
Neuroscience of Comprehension
Lateralization of language
Lateralization of language has frequently been ascribed to a specific side of the brain. There is a lot
of evidence that each brain hemisphere has its own distinct functions. Most often, the right hemisphere
is referred to as the non-dominant hemisphere and the left is seen as the dominant hemisphere. This has
lead to the assumption that the right side of the brain may only be important for receiving sensory
information from the left side and for controlling motor movement of the left half of the body. Yet,
though it appears that it does not possess many language abilities, but is rather necessary for spatial
tasks and non-verbal processing, this does not mean that both brain halves do not work together, in
order to achieve maximal function. On the contrary, if interhemispheric transport is not hindered in
some way or another, both halves can effectively interact with one another.
Anatomical differences between left and right hemisphere
Initially we will consider the most apparent part of a differentiation between left and right
hemisphere: Their differences in shape and structure. As visible to the naked eye there exists a clear
asymmetry between the two halves of the human brain: The right hemisphere typically has a bigger,
wider and farther extended frontal region than the left hemisphere, whereas the left hemisphere is
bigger, wider and extends farther in it’s occipital (backward) region (M. T. Banich,“Neuropsychology“,
ch.3, pg.92). Significantly larger on the left side in most human brains is a certain part of the temporal
lobe’s surface, which is called the planum temporale. It is localized near Wernicke’s area and other
auditory association areas, wherefore we can already speculate that the left hemisphere might be
stronger involved in processes of language and speech treatment. In fact such a leftlaterality of
language functions is evident in 97% of the population (D. Purves, „Neuroscience“, ch.26, pg.649). But
actually the percentage of human brains, in which a „left-dominance“ of the planum temporale is
traceable, is only 67% (D. Purves, „Neuroscience“, ch.26, pg.648). Which other factors play a role
here, and lead to this high amount of human brains in which language is lateralized, is simply not clear.
Functional asymmetry
A rarely performed but popular surgical method to reduce the frequency of epileptic seizures in
hard cases of epilepsy is the so called corpus callosotomy. Here a radical cut through the connecting
„communication bridge“ between right and left hemisphere, the corpus callosum, is done; the result is a
„split-brain“. For patients whose corpus callosum is cut, the risk of accidental physical injury is
mitigated, but the side-effect is striking: Due to this eradicative transection of left and right half, these
two are not longer able to communicate adequately. They function for their owns, separated and
disjoined. This situation provides the opportunity to study the functionality of the two hemispheres
independently. First experiments with split-brain patients were performed by Roger Sperry and his
colleagues at the California Institute of Technology in 1960 and 1970 (D. Purves, „Neuroscience“,
ch.26, pg.646). They lead researchers to sweeping conclusions about laterality of speech and the
organization of the human brain in general.
In split-brain experiments it is typically made use of the laterality of the visual system: A visual
stimulus, located within the left visual field, projects onto the nasal (inner) part of the left eye’s retina
and onto the temporal (outer) part of the right eye’s retina. As images on the temporal retinal region are
to be processed in the visual cortex of the same side of the brain (ipsilateral), whereas nasal retinal
information is mapped onto the opposite half of the brain (contralateral), the stimulus within the left
Wikibooks | 95
Chapter 10
visual field will completely arrive in the right visual cortex to be processed and worked up. In
„healthy“ brains this information furthermore attains the left hemisphere via the corpus callosum and
can be integrated there. In split-brain patient’s brains this current of signals is interrupted; the stimulus
remains „invisible“ for the left hemisphere.
Now in such an experiment a visual stimulus is often produced for only one half of the brain (that
is, within one –the opposite- half of the visual field), while the participant is instructed to name the seen
object, and to blindly pick it out of an amount of concrete objects with the contralateral hand. It can be
shown that a picture, for example the drawing of a die, which was only been presented to the left
hemisphere, can be namend by the participant („I saw a die“), but is not selectable with the right hand
(no idea which object to choose from the table). Contrarily the participant is unable to name the die, if
it was seen by the right hemisphere, but easily picks it out of the heap of objects on the table with the
help of the left hand.
These outcomes are clear evidence of the human brain’s functional asymmetry. The left
hemisphere seems to dominate functions of speech and language processing, but is unable to handle
spatial tasks like vision-independent object recognition. The right hemisphere seems to dominate
spatial functions, but is unable to process words and meaning. In a second experiment it can be shown
that a split-brain patient can only follow a written command (like „get up now!“), if it is presented to
the left hemisphere. The right hemisphere can only „understand“ pictorial instructions. The following
table (D. Purves, „Neuroscience“, ch.26, pg.647) gives a distinction of functions:
Left Hemisphere
Right Hemisphere
• analysis of right visual
field
• analysis of left visual field
• spatial tasks
• language processing
• visuospatial tasks
• writing
• object and face recognition
• speech
It is important to keep in mind that these distinctions comprise only functional dominances, no
exclusive competences. In cases of unilateral braindamage, often one half of the brain takes over tasks
of the other one; full effectiveness of the two hemispheres is only reached during constructive
interaction of both. So, it would be a fallacy to conclude the right hemisphere to have completely no
influence on speech and language processing. One of the next sections will go into this point.
Cognitive functioning is most often ascribed to the right hemisphere of the brain. When damage is
done to the this part of the brain or when temporal regions of the right hemisphere are removed, this
can lead to cognitive-communication problems, such as impaired memory, attention problems, and
poor reasoning (L. Cherney, 2001). Investigations lead to the conclusion that the right hemisphere
processes information in a gestalt and holistic fashion, with a special emphasis on spatial relationships.
Here, an advantage arises for differentiating two distinct faces because it examines things in a global
manner and it also reacts to lower spatial, and also auditory, frequency. The former point can be
undermined with the fact that the right hemisphere is capable of reading most concrete words and can
make simple grammatical comparisons (M. T. Banich,“Neuropsychology“, ch.3, pg.97). But in order to
function in such a way, there must be some sort of communication between the brain halves. Since
1990, research suggests that the hemispheres do not have a single way of interacting with each other
but can do so in a variety of ways. The corpus callosum, as well as some subcortical comissures serve
for interhemispheric transfer. Both can simultaneously contribute to performance, since they use
96 | Cognitive Psychology and Neuroscience
Neuroscience of Comprehension
complement roles in processing.
Handedness
An important issue, when exploring the different brain organization, is handedness, which is the
tendency to use the left or the right hand to perform activities. Throughout history, left-handers, which
only comprise about 10% of the population, have often been considered being something abnormal.
They were said to be evil, stubborn, defiant and were, even until the mid 20th century, forced to write
with their right hand. An example that shows their initial position in society is the latin word sinistra,
which means left, as well as unlucky, or an indian tradition, where the left hand is reserved for
bathroom functions (M.T.Banich, "Neuropsychology", ch.3, pg. 117). There are many negative
connotations associated with the phrase "being left-handed", e.g. being clumsy, awkward, insincere,
malicious, etc.
One most commonly accepted idea, as to how handedness affects the hemispheres, is the brain
hemisphere division of labor. Since both speaking and handiwork require fine motor skills, its
presumption is that it would be more efficient to have one brain hemisphere do both, rather than having
it divided up. Since in most people, the left side of the brain controls speaking, right-handedness
predominates. The theory also predicts that left-handed people have a reversed brain division of labor.
In right handers, verbal processing is mostly done in the left hemisphere, whereas visuospatial
processing is mostly done in the opposite hemisphere. Therefore, 95% of speech output is controlled by
the left brain hemisphere, whereas only 5% of individuals control speech output in their right
hemisphere. Left-handers, on the other hand, have a heterogeneous brain organization. Their brain
hemisphere is either organzied in the same way as right handers, the opposite way, or even such that
both hemispheres are used for verbal processing. But usually, in 70% of the cases, speech is controlled
by the left-hemisphere, 15% by the right and 15% by either hemisphere. When the average is taken
across all types of left-handedness, it appears that left-handers are less lateralized.
After, for example, damage occurs to the left hemisphere, it follows that there is a visuospatial
deficit, which is usually more severe in left-handers than in right-handers. Dissimilarities may derive,
in part, from differences in brain morphology, which concludes from asymmetries in the planum
temporale. Still, it can be assumed that left-handers have less division of labor between their two
hemispheres than right-handers do and are more likely to lack neuroanatomical asymmetries
(M.T.Banich, "Neuropsychology", ch.3, pg. 123).
There have been many theories as to find out why people are left-handed and what its
consequences may be. Some people say that left-handers have a shorter life span or higher accident
rates or autoimmune disorders. According to the theory of Geschwind and Galaburda, there is a relation
to sex hormones, the immune system, and profiles of cognitive abilities that determine, whether a
person is left-handed or not. Concludingly, many genetic models have been proposed, yet the causes
and consequences still remain a mystery (M.T.Banich, "Neuropsychology", ch.3, pg. 119).
Wikibooks | 97
Chapter 10
Auditory Language Processing
For understanding how language is organized
neurologically and what its fundamental components are,
brain lesions, namely aphasiae, are examined. We will first
consider the neurological perspective of work with aphasia
and then turn to the psychological perspective later on in the
chapter.
Neurological Perspective
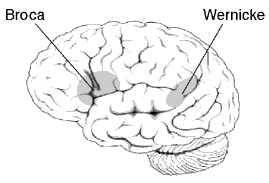
Broca's and Wernicke's area
One of the most well-known aphasiae is Brocàs aphasia, that causes patients to be unable to
speak fluently, but rather have a great difficulty producing words. Comprehension, however, is
relatively intact in those patients. Because these symptoms do not result from motoric problems of the
vocal musculature, a region in the brain that is responsible for linguistic output must be lesioned. Broca
found out that the brain region causing fluent speech is responsible for linguistic output, must be
located ventrally in the frontal lobe, anterior to the motor strip. Recent research suggested that Brocàs
aphasia results also from subcortical tissue and white matter and not only cortical tissue.
Another very famous aphasia, known as Wernickès aphasia, causes the opposite syndromes as
described above. Patients suffering from Wernickès aphasia usually speak very fluently, words are
pronounced correctly, but they are combined senselessly – “word salad” is the way it is most often
described. Understanding what patients of Wernickès aphasia say is especially difficult, because they
use paraphasiae (subsitution of a word in verbal paraphasia, of word with similar meaning in semantic
paraphasia, and of a phoneme phonemic paraphasia) and neologisms.With Wernickès aphasia
comprehending simple sentences is a very difficult task. Thus their ability to process auditory language
input but also written language is impaired. Concluding from this, one can say that the area that causes
Wernickès aphasia, is situated at the joint of temporal, parietal and occipital regions, near Heschl`s
gyrus (primary auditory area), because all the areas receiving and interpreting sensory information
(posterior cortex), and those connecting the sensory information to meaning (parietal lobe) are likely to
be involved.
Wernicke did not only detect the brain region responsible for comprehension, but also concluded
that with an impairment of the brain region betwenn Wernickès and Brocàs area, speech could still be
comprehended and produced, but repeating just heard sentences could not be possible, because the
input received could not be conducted forwarded to Brocàs area to be reproduced. Thus the damage in
this part of the brain is called conduction aphasia. Research has shown that damage to a large never
fibre tract, the arcuate fasciculus, the connection between the two intact brain regions, causes this kind
of aphasia. That is why conduction aphasia is also regarded as a disconnection syndrome ( behavioural
dysfunction because of a damage to the connection of two connected brain regions).
Transcortical motor aphasia, another brain lesion caused by a connection disruption, is very
similar to Brocàs aphasia, with the difference that the ability to repeat is kept. In fact people with a
transcortical motor aphasia often suffer from echolalia, the need to repeat what they just heard. Usually
patients` brain is damaged outside Brocàs area, sometimes more anterior and sometimes more
superior. Individuals with transcortical sensory aphasia have similar symptoms are those suffering
from Wernickès aphasia, except that they show signs of echolalia.
98 | Cognitive Psychology and Neuroscience
Neuroscience of Comprehension
Lesions in great parts of the left hemisphere lead to global aphasia, and thus to an inability of both
comprehending and producing language, because not only Brocàs or Wenickès area is damaged.
(Barnich, 1997, pp.276-282)
Spontaneous
Type of Aphasia
Paraphasia
Comprehension Repetition
Naming
Speech
• Uncommo
• Poor
• Nonfluen
• Brocàs
n
t
• Poor
• Wernickès
• Common
• Good
• Poor
• Poor
• Fluent
• Conduction
(verbal)
• Poor
• Good
• Poor
• Fluent
• Transcortica
• Common
• Good
(echolali
• Poor
l motor
• Nonfluen
(literal)
a)
t
• Good
• Poor
• Transcortica
• Uncommo
• Poor
• Good
• Poor
l sensory
• Fluent
n
• Poor
(echolali
• Poor
• Nonfluen
• Global
a)
t
• Common
• Variable
• Poor
(Adapted from Benson, 1985,p.32 as cited in Barnich, 1997, p.287)
Psychological Perspective
Examining from the psychological perspective, brain lesions are used to understand which parts of
the brain play roles for the linguistic features phonology, syntax and semantics.
Phonology
Examining which parts are responsible for phonetic representation, patients with Brocàs or Wernickès aphasia can be compared. As the speech characteristic for patients with Brocàs aphasia is
non-fluent, i.e. they have problems prodcuing the correct phonetic and phonemic representation of a
sound, and people with Wernickès aphasia do not show any problems speaking fluently, but also have
problems producing the right phoneme. This indicates that Brocàs area is mainly involved in
phonological production and also, that phonemic and phonetic representation do not take place in the
same part of the brain. Scientists examined on a more precise level of speech production, on the level
of the distinctive features of phonemes, to see in which features patients with aphasia made mistakes.
Results show that in fluent as well as in non-fluent aphasia patients usually mix up only one distinctive
feature, not two. In general it can be said that errors connected to the place of articulation are more
common than those linked to voicing. Interestingly some aphasia patients are well aware of the
different features of two Phoneme phonemes, yet they are unable to produce the right sound. This
suggests that though patients have great difficulty pronouncing words correctly, their comprehension of
words is still quite good. This is characteristic for patients with Brocàs aphasia, while those with
Wernickès aphasia show contrary symptoms: they are able to pronounce words correctly, but cannot
understand what the words mean. That is why they often utter phonologically correct words
(neologisms), that are not real words with a meaning.
Syntax
Wikibooks | 99
Chapter 10
Humans in general usually know the syntax of their mother tongue and thus slip their tongue if a
word happens to be out of order in a sentence. People with aphasia, however, often have problems with
parsing of sentences, not only with respect to the production of language but also with respect to
comprehension of sentences. Patiens showing an inability of comprehension and production of
sentences usually have some kind of anterior aphasia, also called agrammatical aphasia. This can be
revealed in tests with sentences, these patients cannot distinguish between active and passive voice
easily if both agent and object could play an active part. For example patients do not see a difference
between “The boy saw the girl” and “The girl was seen by the boy”, but they do understand both “The
boy saw the apple” and “The apple was seen by the boy”, because they can seek help of semantics and
do not have to rely on syntax alone. Patients with posterior aphasia, like for example Wernickès
aphasia, do not show these symptoms, as their speech is fluent. Comprehension by mere syntactic
means would be possible as well, but the semantic aspect must be considered as well.
Semantics
It has been shown that patients suffering from posterior aphasia have severe problems
understanding simple texts, although their knowledge of syntax is intact. The semantic shortcoming is
often examined by a Token Test, a test in which patients have to point to objects referred to in simple
sentences. As might have