PARTICIPANTS’ FEEDBACK
I am sharing the feedbacks given by the participants of the workshops. I am reproducing the content mostly as shared with minimal copy editing.
Cognitive Drill Therapy is a novel therapy specifically designed for patients of OCD and phobia. Structured over three days, the workshop balanced the theoretical and practical aspects of cognitive drill.
Day-1: Majorly focused on two things. Firstly some cases of OCD and Specific Phobias were shared which helped us to conceptualize the chief complaints of the patients. We understood in detail as to how these problems affect the everyday life of such patients and what all attempts are made by them to cope up with their problems. Secondly, the focus was on the basic principles of Classical Conditioning. It helped us to understand the application of underlying principles of classical conditioning in development of OCD and phobia. The distinction between unconditioned and conditioned stimulus could well be connected to covert and overt structures. The surface structure needs to be explored for underlying structures. Response generalization takes place gradually so that each patient develops his own ‘umbrella’ of causes, meaning that many stimuli elicit the same anxiety response. Day-1 gave all of us enough food for thought and we could appreciate that the suffering of an OCD patient or a phobic might seem very casual to an outsider but it is very genuine for the patient.
Day-2 was power packed as it focused on the implementation. Though individual differences can exist, but on an average, a patient requires about 10 sessions of CDT with daily homework. The important aspects covered on day-2 were as follows:
Case History: The major aim of the case history is to gather detailed background, discovering conditioned stimuli, underlying fear structures, attempts made by the patient to cope with the problem and how the patient’s life has been affected by all this. The most pertinent question during this enquiry phase probably is ‘what do you think will happen if …….’ ?
Assessment: It refers to administration of standardized tools to objectively assess the reported fears and anxiety. Depending upon the requirement one can use Y-BOCS, Fear inventory and any other relevant scale along with a visual analogue scale to get a subjective rating of anxiety felt by the patient.
Psycho-education: This is one of the most important stages of CDT. The patient needs to know the exact diagnosis of the problem followed by the information on the functional nature of the connection between the conditioned stimuli (triggers) and reactions (fear, anxiety). The compulsive actions are a form of avoidance which have been providing a temporary relief to the patient. As a result the problem has persisted and probably worsened over the course of time. CDT works on two basic principles. Firstly, during exposure anxiety follows the pattern of a bell shaped curve which means that it rises, attains a peak and declines thereafter. Secondly, sufficient and repeated exposure to conditioned stimuli tends to reduce its strength.
Cognitive Drill: The final phase is the cognitive drill. The identified triggers are converted into past or present tense and repeated by the patient till a particular triggers stops eliciting the anxiety response. Each trigger should approximately take about 5-10 minutes. Visual analogue scale is used with each trigger multiple times to assess the intensity of the response. In one session we move on from one CS to another as per the comfort of the patient. The drill is effective when it addresses underlying structures, is multi modality and most important if the patient experiences the anxiety when presented with the stimulus.
Day-2 exposed us to the intricacies of CDT. Detailed case history was demonstrated live and also through reported cases. Information received in case history was kept safe for the final day for drill demonstration.
Day-3 began with live demonstrations of the drill on one of the participants who reported anxiety in a specific performing situation where there was no cue to refer to. The fear of going blank and being embarrassed in front of the audience and associated fears were taken up in the drill. The results confirmed the efficacy of the drill. The procedural issues became very clear on day three.
Over and above the most important take home points that I would like to mention are:
i. The relevance of Classical Conditioning procedures in learning and unlearning fear responses.
ii. The T-R connection
iii. Breaking down of behavior units into surface and underlying structures
iv. The importance of psycho-education
v. The importance of continuing medicinal support
vi. Multimodality and daring in drill
OCD and specific phobias are probably the disorders with the highest rates of prevalence. The three days workshop was an intense training program which completely changed my outlook on these disorders. The highly structured course material and the focused delivery of that course material worked towards enhancing my knowledge. From the first day on to the third day it was an upward graph as far as learning and understanding is concerned. The program strengthened my understanding of theoretical concepts and raised my conviction for the practical application of the basic principles of classical conditioning. Such programs are add-on to the skill repertoire of any professional working in the field of psychotherapy.
The three days of intense learning were really empowering. From theoretical to practical, from other cases to self, I felt more competent in being able to handle the anxiety issues of my clients. Anxiety is such a natural response that one does not realize when and how it becomes attached to so many stimuli to which it is not a natural response. The abreaction and the cathartic responses that I saw in the in-person training was a wonderful negation of my own apprehensions that how can seemingly funny repetitions of a phrase lead to reduced anxiety. The workshop gave me an opportunity to revisit the theoretical aspects of classical conditioning theory, and helped me to learn the power of sufficient and continued exposure of conditioned stimulus in reducing the associated response of anxiety. From interviewing effectively to explore the underlying issues to prepare the drill for various conditions, the learning is magnanimous.
Workshop on cognitive drill therapy was an amazing learning experience. It was spread into three days, where on day 1 different cases were told to us of Anxiety, Phobia and OCD. We were taught of different complaints that patients make in different mental conditions. How do they react in such a state? How do these anxiety states affect their personal, professional and social life? We also learned that behind cognitive drill therapy, one of the theories that functions is the Pavlovian Conditioning theory. The functioning of classical conditioning which is mainly about stimulus and response was explained. How anxiety or phobic responses develop in a person and how such anxious responses get strengthened and how can we break this connection with the help of cognitive drill therapy. We also learned that whatever symptoms we are able to see or reported by the patient they are the overt level and it has a covert connecting cause to it. So it’s important to identify it.
On day-2, we learnt about the whole process. How should we start the session? So as the person comes with a problem we should take the case history like what all problems he has, since when he has this problem, how does it affects him, what are the disadvantages, what has he done till now to control or treat his problem. Also explore the overt and covert stimulus or causes that create anxiety. During the history taking session we have to identify all the stimuli that cause anxiety in the person and make a list of it so that all the stimuli can be dealt with during the therapy sessions.
Then after taking the detailed case history, we conduct tests for assessment of Anxiety, Fear, OCD and also use the Visual Analogue Scale to assess the level of anxiety for each conditioned stimulus. After the assessment of the patient next step is to psycho-educate the person about his illness or disorder where we have to tell the person the diagnosis of his problem and how has the problem developed (that can be done by explaining the Stimulus-Response-Avoidance theory). So these three steps case history, assessment and psycho-education has to be done on the first day when the patient comes.
On the second day of the therapy when we have identified all the triggers and reactions we start up with the Cognitive drill therapy in which the person has to keep repeating the statement that has been identified as anxiety arousing in past or present tense. Reason being that anxiety is future oriented and person tends to avoid such stimuli which he assumes will cause him pain so starts avoiding them or do not confront them. Avoiding such stimuli which creates anxiety in the person gives the person a temporarily relief and that becomes a pattern. So in CDT person will repeat the statement in the present or past tense form which as a result will increase his anxiety gradually, will go higher and then gradually will go down(forming the bell shaped curve).This bell shaped curve is also a proof that you are working on the correct stimulus. While doing drill we have to involve lot of sensory modalities like patient will himself repeat the statement that is verbal, therapist repeats the statement and the patient listens to it that’s auditory, patient writes the statement down that’s kinesthetic.
While doing the drill patient has to visualize the situation as vividly as possible so that he experiences the same anxiety as if it is real. Along with the drill, if possible then we have to dare the patient to either touch the object or to get in close proximity with the feared object. Along with drill and dare we also have to tell the person to distract himself from these anxious thought by getting engaged into his daily activities or social activities because by not doing so person is reinforcing his obsessive or phobic thoughts and giving undue importance to them, So if the person will engage himself into some work or activity will not give unnecessary importance to them. We also have to give homework to the patient for practicing these statements at home. These drill dare and distraction sessions will continue till the time all the stimulus have been practiced and have lost their anxiety arousing feature and have become neutral.
On day-3 we got a chance to see a live demonstration of CDT, as two of the participants volunteered for working upon their anxieties. One of them was a case of social phobia and another had performance anxiety. So we learned about the practical application of the Cognitive Drill Therapy that we had learned in two days in theory form. Watching a demonstration gave much more clarity to the concepts and brought the realization about the power of this technique. Along with the therapy we also have to encourage the patient to take medication and not to leave it without doctor’s consultation. Patient’s family members are also to be psycho-educated about the patient’s illness and therapist can teach the drill to one of the family members so they can help the patient in practicing at home. The therapy has to be practiced for 10-15 days. It will start showing its effect within this period.
Dr. Jain is known for his unique expertise of offering, professionals as well as patient friendly therapeutic interventions. He artistically converts complicated therapies into concise therapeutic models, and effortlessly trains his trainees and transforms them into skilled professionals.
Continuing with the trend of presenting complicated therapeutic interventions in concise capsules Dr. Jain has developed a breakthrough therapy ‘Cognitive Drill Therapy (CDT)’ for the patients with OCD, Phobia and panic attacks. OCD is a chronic disorder and is considered a common psychiatric condition. Treatment of OCD typically involves the use of Psycho- education, pharmacotherapy especially serotonin reuptake inhibitors (SRIs), behavior therapy and cognitive therapy. Cognitive behavior therapy (CBT)/Exposure response prevention (ERP) is considered first line treatment for OCD patients. As Clinical Psychologists across the world know very well that treating OCD, Phobia and panic attacks is lengthy treatment irrespective of the therapeutic model preferred by the professionals, and significant improvement in the illness is also not perceived by some patients which lead to significant dropouts.
Dr. Jain while working with an adult with chronic OCD, had illuminative thought of cognitive drill as therapy. The cases of OCD treated with cognitive drill in combination with pharmacotherapy have been instrumental in establishing CDT as a potentially rapid therapy for treatment of OCD/phobia. He initially prescribes a 10 days course in OCD which can be repeated as per the requirements of the patients. However, in cases of Phobias it usually needs less than10 days course of Cognitive Drill Therapy. He is demonstrating success of Cognitive Drill Therapy in various phobias including social anxiety, agoraphobia and specific phobias. Also it is observed that a simple listening to his approach of Cognitive Drill Therapy, a few patients integrated it into their lives and got improved without explicit and interactive focused sessions with Dr. Jain.
On the first day of the training we were skeptical of success of the CDT in OCD and phobia, social anxiety and panic attack patients per se. We underwent the first day training with skeptical thoughts laden with our own fear of failure to treat OCD originating out of our past experiences with OCD patients. When a larva comes out of its cocoon and converts into an ugly caterpillar no one can imagine that the same ugly caterpillar will transform into a beautiful butterfly. This was the experience of each and every student after completing the three days training. We were transformed into a confident professionals bubbling with energy and conviction to treat disorders like OCD, social anxiety, panic attacks, phobia in just 1 hour per day for 10 days on an average, depending on severity of the case. The OCD patients however, may need longer time depending upon the severity. Dr. Jain is very clear that this therapy cannot treat 100% patients with equal level of success and no unrealistic claims of absolute recovery from these disorders is claimed. However, the applications of Cognitive Drill Therapy do produce significant improvement rapidly in many cases.
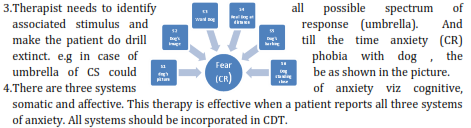
Day 1- Understanding theoretical perspective: On day-1 Dr. Jain oriented us towards new perspective on application of Pavlovian theory of conditioning for extinction of the fear (conditioned responses) with various stimulus of obsession (CS). We were also sensitized that thoughts associated with CS in case of phobia/social anxiety/OCD are originate in brain centers which are responsible for future tenses. OCD patients speculate the consequences of obsessive thought and to avoid the harm and the pain develop various anxiety and fear; and by making a patient do cognitive drill, we symbolically align the patient’s brain and in turn get benefited rapidly through following mechanism-
1. Neural pathways of brain (centre of future tense) diminishes responsible for OCD/ anxiety disorder
2. The fear/crystallized anxiety (CR) extinct in absence of UCS stimuli.
3. Patient does cognitive reinterpretation of the fear , underlying themes and attains self efficacy
A few important component of CDT were also elaborated.
1. Anxiety on stimulus can be elicited by its mere mental representation (Covert conditioned stimulus). The process is as follows Covert stimulus covert response (Neural firing & Release of hormone)
2. Emotionally charged words act as conditioned stimulus and has potential to elicit conditioned response (fear/ anxiety). Mere repeating of the conditioned stimulus/word will elicit fear and after a period of time when anxiety (CR) will reach to its peak, it will decline.
5. The therapist should prefer all modalities for CDT e.g taking patient to real site, writing, imagining and auditory.
Day 2- Case studies and experiential learning through CDT session on one of the trainee suffering with social phobia: The theoretical perspectives we learned on day-1 were explained by Dr. Jain with supporting case studies. CDT was demonstrated on one of the participants who was having stage phobia. Steps were as following-
1. Taking relevant case history
2. Taking problem statements
3. Identifying underlying themes (umbrella). Make him aware that CDT doesn’t eliminate anxiety, but it disconnects the connection between stimulus (feared stimulus) and fears (conditioned response).
4. Identifying three modalities of anxiety viz cognitive, affective and somatic.
5. Psycho-educate the patient about CDT on following aspects-
A. Meaning of the illness
B. Three types of anxiety reactions – fight, flight, freeze. We react to feared stimulus by avoidance thereby we avoid.
C. Fear has many underlying themes/issues which need to be addressed. Identifying the umbrella of stimuli is required. The patient avoids object/stimulus which only give temporary relief from fear, thus real issues are never addressed. e.g A student might be avoiding giving presentation, because he has underlying fear that he may be ridiculed, looked down upon if he makes mistake
D. Fear has future orientation in brain. By changing the orientation from future to past or present during CDT the neural pathway of fear breaks down in brain.
E. Fear has its cycle. After reaching its peak fear/anxiety diminishes
F. Importance of medicine/pharmacotherapy in treatment of OCD. He encourages combination treatment in OCD. Medicine recommendations are invariably made through psychiatric consultations.
G. CDT is three component therapy- Drill, Daring & Distraction.
H. Patients should also be told that all existing OCD themes will extinct after therapy but new themes may develop over the period of time, same therapy can be used.
I. Patients should be psycho-educated for giving NIL Importance to their OCD thoughts and study about OCD as much as possible. He may be recommended to read book ‘brain lock’ which illustrates OCD is due to thoughts locked in brain.
6. Following test to be taken pre & post CDT
A. Narration from patient about illness
B. Visual Analogue Scale
C. Subjective Reports of Distress
D. Depending on the case, pre and post CDT tests to administer on the patient. For OCD patients YBOC, Generalized anxiety scale, fear inventory, etc can be used
7. CDT Session: Practice session may continue for 10 days (1hr /day plus Home Work). Therapist should make patient perform drill for all stimulus in umbrella using as many modalities as possible (speaking, writing, listening, imagining, and seeing in real). When patient ceases to exhibit anxiety, he should be asked to perform a daring act by facing the feared stimulus in real. If patient doesn’t exhibit anxiety; the drill on that stimulus can be terminated as it’s the indicator of extinction of anxiety (CR)
A. 1 hour CDT to be done at clinic.
B. Each trigger of anxiety to be given 10-15 min approx. All modalities of stimulus presentation viz. visual, auditory, writing and tactile should be used.
C. Report on level of anxiety to be taken every 30 second.
D. Patient should be given Homework to do CDT at home. He should be advised to keep himself distracted means engaged professionally/socially.
Day-3: Day for skill refinement on CDT: On day-3 feedback was taken from the participant, who had been given the CDT for her stage fear on previous day. It was amazing to witness her cognitive restructuring on her stage fear. It was surprising to notice that she was laughing at her irrational themes of fear. Unbelievably, we also noticed her enhanced self-efficacy. The same participant, who was shivering while narrating her fear, had reframed her thoughts on stage fear. The same participant later reported that after three days she gave a live performance before huge audience without any sign of stage fear
Last day CDT was demonstrated on other participant who was having anxiety for public speaking. Patient of OCD will have many stimulus of anxiety whereas patient of phobia will have limited anxiety.
We all felt skilled and empowered. I also applied Cognitive Drill Therapy by my own and observed extra-ordinary improvement in the condition of the recipients. I am excited to extend its applications as and when I get cases on which this novel and highly effective form of psychotherapy is indicated.
After completing a three days workshop on CDT conducted by Dr. Rakesh Jain , First and foremost, I want to say that we Indian psychologists should feel proud on Dr. Jain for developing a new therapy. It is evident that Cognitive drill therapy will prove an excellent therapy for treatment of as complicated disorder as phobias, OCD and anxiety disorders in future. Dr. Jain made it very simple and logical and also taught us in a very effective manner. I personally recommend that it should be learnt by all psychologists as well as psychiatrists. God bless him to keep this sprit for developing other contributions.
I would like to place on record my sincere gratitude to Dr Jain for giving a soldier an exposure to such a path breaking therapy - CDT which accords an opportunity not only to professionals of this field, but to one and all to make a difference in combating the most common and widespread situation relating to mental health such as OCD and Phobias. The 3 day workshop under Dr Jain's guidance and interaction with wonderful participants was an experience akin to opening of 'chakras'. The uniqueness of CDT motivates us "to go beyond the call of duty" because "If you only do what you can do, you will always remain where you are".
All of us are doing well in life but in some areas we are unable to perform to out inherent potential. What limits us is our “Fears”. There are many varieties of fears e.g. fear of enclosed spaces, fear of rejection, fear of failure, fear of success, fear of rats etc. Fear is something about imagined consequences. CDT is a great low-cost therapy that helps us clear our quickly and efficiently by “facing it”. This therapy destroys the underlying structure totally and completely. As a matter of fact CDT empowers people so that they can clear any new fears they develop in future on their own. CDT reminds me of the famous ad line “DARR KE AAGYE JEET HAI”.
Sir, I think that CDT workshop makes us very resourceful in the area of treating phobia and OCD. My own experience as a subject was wonderful. So I am very much assured about its results and now I preferred CDT as my first choice of treatment. Sir, you explain all the concepts of CDT in very easy and simple words. Sir, CDT workshop was really wonderful. I am very thankful to for this workshop.
I am proud of being a student of psychology and fortunate to have a 'GURU' like Dr. JAIN SIR. When I heard about CDT, I became eager to know about it. The workshop, organized by Dr. Jain Sir, always attracted me because he has ability to impregnate the knowledge of the topics in our mind in very simple way. I could not resist myself to attend the workshop on CDT. This workshop described systematic procedure of CDT to us, enhanced our therapeutic knowledge to treat the patients by cognitive restructuring and enabled us to make research plans in this area. In this workshop, we could know about hidden, underlying structure of fear. We learned that CDT would help us to treat the patients and we would be capable to enable them to deal with their fear/obsession by 'Soch to Soch' (thinking to thinking) and to get rid of their unnecessary behavior in real life. Thus CDT is a structured way to cope up from fear by verbal exposure. I am thankful to Dr. Jain Sir who is not only my teacher but also enlightened my line of career as a psychotherapist
Most of the participants feel empowered within a span of 2-3 days. They can successfully conceptualize the concepts and applications of Cognitive Drill Therapy and can execute the same on the patients suffering from phobic/OCD conditions.
--x--