123
Student Lesson 4
L E S S O N 5
Elaborate/Evaluate
Drug Addiction Is a
Disease—So What
Do We Do
about It?
Photo courtesy of Gray Wolf Ranch Wilderness Recovery Lodge.
Overview
At a Glance
Students make predictions about the success rate for treatment of addiction
compared with treatment for other chronic diseases. Then students evaluate
case studies of individuals with different diseases to compare and contrast
how the diseases are similar to, or different from, the others.
Major Concept
Drug addiction is a recurring chronic disease that can be treated effectively,
similar to other chronic diseases.
Objectives
By the end of these activities, the students will
• understand that addiction is a chronic disease that is likely to recur;
• recognize that treatment is most effective when it combines medication
and behavioral treatments;
• be able to explain how treatment for addiction is similar to that for
other chronic diseases, such as diabetes or heart disease; and
• recognize that even though we may think that treatment could be
more effective when people who are addicted to drugs, like people with
other chronic diseases, choose to participate actively in their treatment,
research shows that treatment can be very effective even when it is
compulsory.
Basic Science–Health Connection
Addiction has many dimensions and disrupts many aspects of a person’s
life. Sci entific research and clinical practice have yielded a variety of
effective approaches to treatment for addiction to certain drugs, such as
heroin. Continuing research is yielding new approaches to developing
medications to treat addiction to other drugs, such as cocaine, for which
no medications are currently available.
125
The Brain: Understanding Neurobiology Through the Study of Addiction
Drug abuse and addiction lead to long-term changes in the brain’s chemistry
Background
and physiology. The changes in the brain cause drug-addicted people
Information
not only to lose the ability to control their drug use, but their addiction
also changes all aspects of their lives. People with drug addiction often
become isolated from family and friends and have trouble in school or
work. In addition, the compulsive need for drugs can lead to significant
legal problems. While the biological foundation for drug addiction does
not absolve an individual from the responsibility of his or her actions,
the stigma of drug addiction needs to be lifted so individuals may receive
proper medical treatment, similar to that for other chronic diseases.1
Addiction is a recurring chronic disease. No cure is available at this time,
but addiction can often be treated effectively. Drug addiction is often viewed
as a lapse in moral character. This value judgment influences how society
deals with the disease, both socially and medically. Unfortunately, because
people, including physicians, have often viewed addiction as a self-inflicted
condition, drug-addicted people have not always received the medical
treatment common for other chronic diseases. Treating addiction requires
more than a “just say no” approach.2
Treatment for addiction can be very effective. Treatment is successful when
the addicted person reduces or abstains from drug use, improves his or her
personal health or social function, and becomes less of a threat to public
health and safety.3 Certain addictions, such as heroin addiction, can be treated
with medications.4,5 Methadone, the most common medication, prevents
craving and withdrawal symptoms in heroin addiction. Methadone is an
opioid-receptor agonist. That is, methadone binds to the opi oid receptor
just as heroin does. Methadone, however, does not produce the euphoria
or “high” that results from heroin use. When taken orally as indicated,
it does not produce the rapid increase in opioid-receptor occupancy that
comes from injecting or snorting heroin, but it does maintain sufficient
opioid-receptor activity to prevent withdrawal and cravings for opioids.
Figure 5.1: Methadone can be part of an effective treatment plan for addiction to
opiates. Photo graph of pills by, and used with permission of, Roxane Laboratories,
Inc. All Rights Reserved.
A second medication prescribed for heroin addiction is naltrexone.
Unlike methadone, naltrexone is an opioid-receptor antagonist. Instead of
competing with or mimicking heroin for the opioid receptor, naltrexone
prevents heroin from binding to the receptor, thereby preventing heroin
126
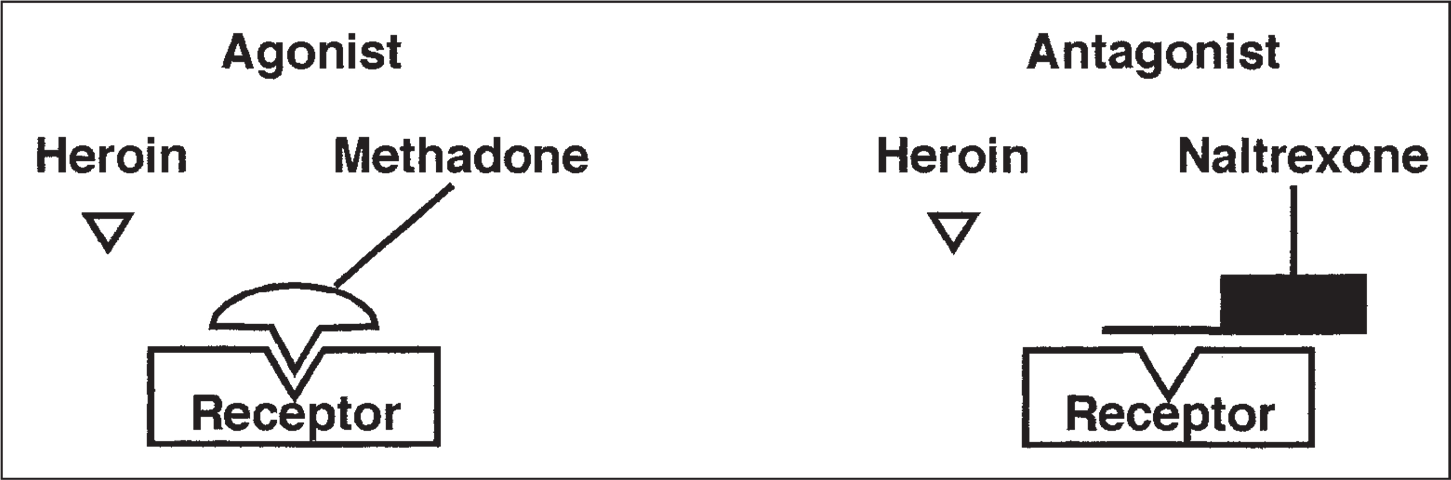
Figure 5.2: Agonists are chemicals that bind to a specific receptor to elicit a response,
such as excitation or inhibition of action potentials. Methadone is an agonist that,
like heroin, binds to opioid receptors. Unlike heroin, however, methadone does not
produce the same level of eupho ria. Buprenorphine is a partial agonist that also binds
to opioid receptors. Partial agonists are chemicals that are similar to full agonists,
but at higher doses their effect is not as great as a ful agonist’s. Buprenorphine does
not produce the euphoria seen with heroin. Antagonists are chemicals that bind
to a receptor and block it, producing no response and preventing other chemicals
(drugs or receptor agonists) from binding or attaching to the receptor. Naltrexone
is an antagonist that binds to the opioid receptor and blocks heroin from binding.
from eliciting the euphoric high (see Figure 5.2). Buprenorphine is also
used to treat heroin addiction. It is a long-acting partial opioid-receptor
agonist. It acts on the same receptors as heroin but does not produce the
same intense “high” or dangerous side effects. Buprenorphine has some
advantages over other medications for treating heroin addiction. Unlike
methadone, buprenorphine can be prescribed in physicians’ offices. It is
also less likely to be toxic or abused than methadone.
Table 5.1 outlines the different medications used to treat addic tion. The
development of medications to treat drug addiction has been diffi cult
because the brain, the main target of addictive drugs, is such a complex
organ. Until scientists understand how drugs affect the chemistry of the
brain, they cannot develop medicines that will alter their effects.
Table 5.1: Medications for Addiction4
Medication
Treatment for addiction to
Mechanism
Methadone
Heroin
Opioid-receptor agonist
Naltrexone
Heroin
Opioid-receptor antagonist
Naloxone
Heroin, alcohol
Opioid-receptor antagonist
Buprenorphine
Heroin
Mixed opioid-receptor agonist
and antagonist
Nicotine gum, patches
Nicotine
Provide low doses of nicotine
Medication, if available, is rarely sufficient for effective treat ment. Behavioral
treatment in combination with medication is the most effective way to treat
drug addiction.6,7 People recovering from drug addiction need to address the
behavioral and social consequences of their drug use and learn to cope
with the social and environmental factors that contribute to their illness.7
Behavioral treatments can be provided either individually or as a group.
127
Student Lesson 5
The Brain: Understanding Neurobiology Through the Study of Addiction
Principles of Effective Drug Addiction Treatment
1. Addiction is a complex but treatable disease that affects brain function and behavior. Drugs of
abuse alter the brain’s structure and function, resulting in changes that persist long after drug
use has ceased. This may explain why drug abusers are at risk for relapse even after long periods
of abstinence and despite the potentially devastating consequences.
2. No single treatment is appropriate for everyone. Matching treatment settings, interventions,
and services to an individual’s particular problems and needs is critical to his or her ultimate
success in returning to productive functioning in the family, workplace, and society.
3. Treatment needs to be readily available. Because drug-addicted individuals may be uncertain
about entering treatment, taking advantage of available services the moment people are ready
for treatment is critical. Potential patients can be lost if treatment is not immediately available
or readily accessible. As with other chronic diseases, the earlier treatment is offered in the
disease process, the greater the likelihood of positive outcomes.
4. Effective treatment attends to multiple needs of the individual, not just his or her drug abuse.
To be effective, treatment must address the individual’s drug abuse and any associated medical,
psychological, social, vocational, and legal problems. It is also important that treatment be
appropriate to the individual’s age, gender, ethnicity, and culture.
5. remaining in treatment for an adequate period of time is critical. The appropriate duration
for an individual depends on the type and degree of his or her problems and needs. Research
indicates that most addicted individuals need at least 3 months in treatment to significantly
reduce or stop their drug use and that the best outcomes occur with longer durations of treatment.
Recovery from drug addiction is a longterm process and frequently requires multiple episodes
of treatment. As with other chronic illnesses, relapses to drug abuse can occur and should signal
a need for treatment to be reinstated or adjusted. Because individuals often leave treatment
prematurely, programs should include strategies to engage and keep patients in treatment.
6. Counseling—individual and/or group—and other behavioral therapies are the most commonly
used forms of drug abuse treatment. Behavioral therapies vary in their focus and may involve
addressing a patient’s motivation to change, providing incentives for abstinence, building
skills to resist drug use, replacing drug-using activities with constructive and rewarding
activities, improving problemsolving skills, and facilitating better interpersonal relationships.
Also, participation in group therapy and other peer support programs during and following
treatment can help maintain abstinence.
7. Medications are an important element of treatment for many patients, especially when
combined with counseling and other behavioral therapies. For example, methadone and
buprenorphine are effective in helping individuals addicted to heroin or other opioids stabilize
their lives and reduce their illicit drug use. Naltrexone is also an effective medication for some
opioid-addicted individuals and some patients with alcohol dependence. Other medications
for alcohol dependence include acamprosate, disulfiram, and topiramate. For persons addicted
to nicotine, a nicotine replacement product (such as patches, gum, or lozenges) or an oral
medication (such as bupropion or varenicline) can be an effective component of treatment
when part of a comprehensive behavioral treatment program.
8. An individual’s treatment and services plan must be assessed continually and modified as
necessary to ensure that it meets his or her changing needs. A patient may require varying
combinations of services and treatment components during the course of treatment and
recovery. In addition to counseling or psychotherapy, a patient may require medication, medical
services, family therapy, parenting instruction, vocational rehabilitation, and/or social and legal
services. For many patients, a continuing care approach provides the best results, with the
treatment intensity varying according to a person’s changing needs.
128
9. Many drug-addicted individuals also have other mental disorders. Because drug abuse and
addiction—both of which are mental disorders—often co-occur with other mental illnesses, patients
presenting with one condition should be assessed for the other(s). And when these problems
co-occur, treatment should address both (or all), including the use of medications as appropriate.
10. Medically assisted detoxification is only the first stage of addiction treatment and by itself
does little to change long-term drug abuse. Although medically assisted detoxification can
safely manage the acute physical symptoms of withdrawal and, for some, can pave the way
for effective long-term addiction treatment, detoxification alone is rarely sufficient to help
addicted individuals achieve long-term abstinence. Thus, patients should be encouraged to
continue drug treatment following detoxification. Motivational enhancement and incentive
strategies, begun at initial patient intake, can improve treatment engagement.
11. Treatment does not need to be voluntary to be effective. Sanctions or enticements from family,
employment settings, and/or the criminal justice system can significantly increase treatment
entry, retention rates, and the ultimate success of drug treatment interventions.
12. Drug use during treatment must be monitored continuously, as lapses during treatment do occur.
Knowing their drug use is being monitored can be a powerful incentive for patients and can help
them withstand urges to use drugs. Monitoring also provides an early indication of a return to drug
use, signaling a possible need to adjust an individual’s treatment plan to better meet his or her needs.
13. Treatment programs should assess patients for the presence of HIV/ AIDS, hepatitis B and C,
tuberculosis, and other infectious diseases as well as provide targeted risk-reduction counseling
to help patients modify or change behaviors that place them at risk of contracting or spreading
infectious diseases. Typically, drug abuse treatment addresses some of the drug-related behaviors
that put people at risk of infectious diseases. Targeted counseling specifically focused on reducing
infectious disease risk can help patients further reduce or avoid substance-related and other
high-risk behaviors. Counseling can also help those who are already infected to manage their
illness. Moreover, engaging in substance abuse treatment can facilitate adherence to other
medical treatments. Patients may be reluctant to accept screening for HIV (and other infectious
diseases); therefore, it is incumbent upon treatment providers to encourage and support HIV
screening and inform patients that highly active antiretroviral therapy (HAART) has proven
effective in combating HIV, including among drugabusing populations.
Source: NIDA. 2009. Principles of Drug Addiction Treatment: A Research-based Guide, 2nd edition. 2009. National Institute on Drug Abuse.
Relapse is a common event for people recovering form drug addiction. In
many ways, relapse should be thought of as a normal part of the recovery
process. A person in recovery is more likely to experience a relapse if he or
she also has other psychiatric conditions, experiences stress, or lacks the
support of family and friends.
Despite the preconceptions and value judgments many people place on
addiction, it is, in many ways, similar to other chronic diseases such as
dia betes and coronary artery disease. Genetic, environmental, and
behavioral components contribute to each of these diseases. Some people
may argue that drug addiction is different because it is “self-inflicted.” As
presented in Les son 4, the initial choice to use drugs is voluntary, but,
once addiction develops, drug use is compulsive—not voluntary. Moreover,
voluntary choices do contribute to the onset or severity of other chronic
diseases as well. For example, a person who chooses to eat an unhealthy
diet and not exercise increases his or her risk for coronary heart disease.
129
Student Lesson 5
The Brain: Understanding Neurobiology Through the Study of Addiction
Successful treatment for any chronic disease necessitates patient compliance
with the prescribed treatment regimen. Adhering to a treatment plan is
diffi cult for those with any chronic disease. Less than 50 percent of people
with diabetes fol low their routine medication plan, and only 30 percent
follow their dietary guidelines.2 Problems adhering to a treatment plan lead
to about 50 percent of diabetic people needing additional medical care
within one year of diagnosis and initial treatment. Similar statistics hold
true for other chronic diseases: approxi mately 40 percent of patients with
hypertension need emergency room treat ment for episodes of extreme
high blood pressure, and only about 30 percent of adult asthma sufferers
take their medication as prescribed. People treated for drug addiction also
commonly relapse during treat ment and recovery, resuming drug use. The
difficulties in following a treatment plan and coping with the stresses of
a chronic disease illustrate how difficult changing human behavior is. The
challenge of adherence is particularly severe in the case of addiction because
this disease implicates and coopts the very same brain substrates that
underlie what we call free will.8 Activities 2 and 3 of this lesson provide
more insight into this topic.
Scientific research is likely to change how drug addiction is treated. Research
to understand how the brain works and how drugs cause changes in the
chemistry and function of the brain may lead to new medications to treat
dis ease. Scientists continue to work on developing medications that relieve
the cravings experienced when drugs are withdrawn. Also, scientific advances
may reveal ways to reverse the long-term functional changes to the brain that
drugs inflict.
Web-Based Activities
In Advance
Activity
Web Component?
1
No
2
Yes
3
No
4
No
Photocopies
For each group of 3 students
For each student
1 copy of Master 5.1, Ruth’s Story*
1 copy of Master 5.2, Mike’s Story*
1 copy of Master 5.3, Carol’s Story*
1 copy of Master 5.4, Disease
* The Web version of Activity 2 is the preferred approach. Copies of Masters 5.1, 5.2, 5.3,
and 5.4 are needed only if the Internet is unavailable for classroom use.
130
Materials
Activity
Materials
Activity 1
overhead projector
Activity 2
computers (optional)
Activity 3
overhead projector
Activity 4
none
Preparation
Arrange for students to have access to computers for viewing the case
studies in Activity 2.
Activity 1: Is Addiction Treatable?
Procedure
1. Begin the activity by holding a classroom discussion about illness
and disease. Ask, “What is a disease?” Ask students to name some
diseases. Write responses on the board.
Students are likely to say a disease is some problem with the body
This activity is intended
that makes a person feel bad. They may also respond that a disease
to be a quick method
is something you see a doctor about or take medicine for. Students
to assess students’ prior
will list a variety of diseases and conditions. If they don’t include
both short-term minor diseases (such as a cold or flu) and long-term
conceptions about treatcomplex diseases (such as diabetes or heart disease), prompt them
ing drug addiction as
with questions such as, Is a cold a disease? Is diabetes?
a disease.
2. Introduce the terms chronic and acute and give examples of chronic
and acute conditions. Categorize the diseases from Step 1 as either
chronic or acute.
Chronic diseases are those that persist over a long period of time, whereas
acute diseases last only a short time but may have a rapid onset and
marked intensity. Diabetes, heart disease, asthma, and cancer are examples
of chronic diseases. Colds, flu, and a broken bone are acute conditions.
3. Ask students to consider whether addiction is chronic or acute.
Have them explain their answer based on what they have learned in
the unit so far. After students recognize that addiction is a chronic
disease, add it to the list of chronic diseases.
Students’ explanations should include something about the changes
that occur in the brain as a result of drug use (Lessons 2, 3, and 4)
and something about the compulsive, nonvoluntary nature of addiction.
131
Student Lesson 5
The Brain: Understanding Neurobiology Through the Study of Addiction
4. Ask, “Do all diseases or illnesses affect people the same way?”
No. Some are longer lasting and require more intervention from
healthcare providers than others. Some require medicines, others
require psychological treatment, and some require both. Students may
give a cold as an example of a short-term illness that doesn’t require a
great deal of treatment and diabetes or heart disease as a longer-lasting
illness that does require a lot of treatment. Students should realize that
there are similarities as well as differences in disease treatment.
5. Hold a class discussion to find out what students know about treatments
for addiction. Probe student understanding of what a person experiences in
treatment, what types of treatments are available, how long treatment lasts,
and whether it is successful. Have students justify their ideas. Accept all
reasonable answers, and record ideas on the board or a blank transparency.
At this stage, students are likely to have many ideas about treatment
for addiction. Some of their ideas will likely be drawn from stories they
have seen on the Internet or from media coverage of celebrities. Their
ideas may also reflect societal perceptions of addiction and may not
include explanations based on the biology of addiction. <