By: Dr. Sunir Kumar
Neurology is an extremely important part of the Internal Medicine Medical Clerkship and ABIM
Board exam. According to the ABIM exam blueprint, Neurology comprises ~4% of the exam.
Pearl # 1: In Neurology questions on the medical school clerkship and ABIM board
exam, nothing helps narrow the diagnosis than the reflexes mentioned in the vignette
Review the slide below for the most high-yield conditions associated with hyperreflexia, normal
reflexes, hyporeflexia, and delayed reflexes and absent reflexes.
51 | P a g e
K N O W M E D G E
Pearl # 2: We’re not trained ophthalmologists but remembering these eye conditions
can add points to your ABIM score
Optic nerve lesion → can lead to complete blindness in the ipsilateral eye (monocular
blindness of the ipsilateral eye)
Optic chiasm lesion → Bitemporal hemianopiacommon in pituitary tumors that
compress the optic chiasm
Optic tract lesion → contralateral homonymous hemianopia
Optic radiation lesion → contralateral homonymous quadrantanopia
Lack of an ipsilateral adduction to a contralateral gaze is a Medial Longitudinal Fasciculus
(MLF) lesion. This condition, which is also known as intranuclear ophthalmoplegia, is seen in
patients who have Multiple Sclerosis.
In normal individuals, if asked to look the right, the right eye should abduct and the left eye
should adduct. If a patient with MS is asked to look to the right (for example), he/she will be
able to abduct the right eye but fails to adduct the left eye → Lesion is Left MLF.
Same concept applies when asked to look to the left. Normally, the left eye will abduct and
the right eye should adduct. In patients with MS, patients lose the ability to adduct the right
eye → Lesion is Right MLF.
Argyll Robertson Pupil → eyes will be able to constrict when the patient focuses on a near
object (eg. bringing fingers to the nose). This is known as accommodation. However, patients
with an Argyll Robertson pupil lose the ability to constrict the eyes when bright light is shined
into their eyes. In a nutshell, the eyes can’t react to light but can accommodate. This condition
is often seen in patients with syphilis.
Marcus Gunn Pupil → This condition is also known as Relative Afferent Pupillary Defect
(RAPD). In normal individuals, when a swinging flashlight test is performed, both the direct
and consensual eye should constrict to light.
52 | P a g e
K N O W M E D G E
With Marcus Gunn pupil, let’s suppose the left eye is affected. If light is shined into the right
eye, both the direct and consensual will constrict. When light is shined into the left eye, both
the direct and consensual eye will seem dilated (lack of constriction) → Shows damage to the
ipsilateral optic nerve.
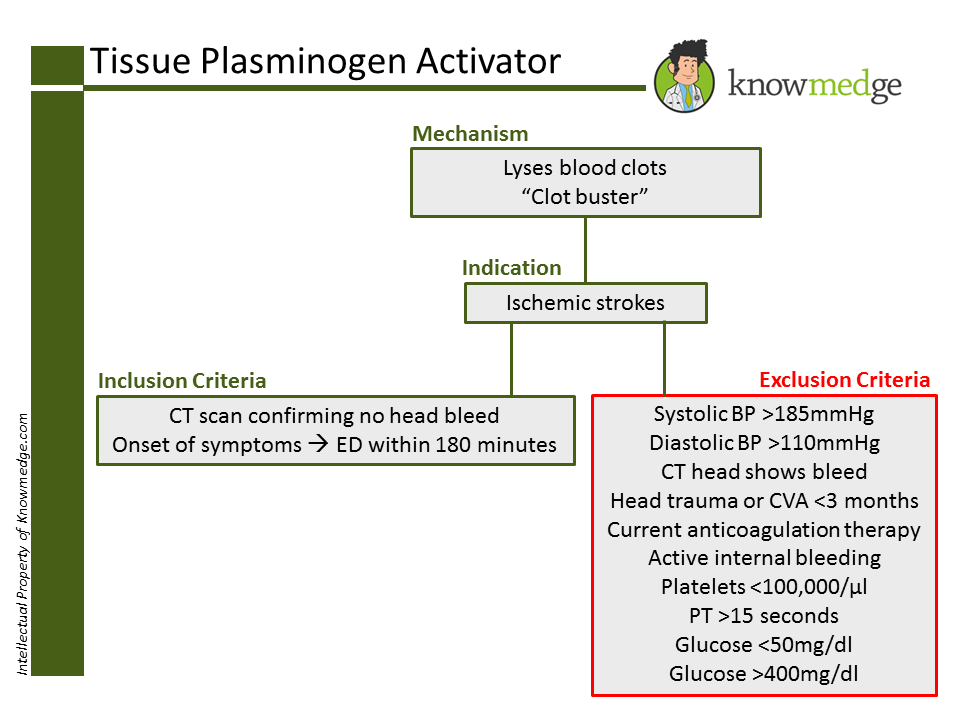
Pearl # 3: Know the indications and contraindications of use of t-PA.
Indications:
o Ischemic stroke as seen on CT head with CLEARLY defined onset of symptoms
o Time of onset of symptoms to administration of t-PA should be no later than 3
hours (180 minutes)
Major Contraindications:
o Blood pressure greater than or equal to 185/110mmHg
o CT head indicates a hemorrhagic stroke rather than an ischemic stroke
o Major trauma to the head within the past 3 months
o Major surgery within the past 14 days
o Current use of anticoagulants as administering t-PA with anticoagulants
increases risk of major bleeds
o Platelet count of less than 100,000/uL
o PT>15 seconds
o Glucose 400 mg/dl
53 | P a g e
K N O W M E D G E
Pearl # 4: Identifying buzzwords is key for selecting the correct neurological diagnosis
when CT/MRI findings are included in the vignette.
Multiple Sclerosis → increased T2 signal and decreased T1 signal. There will be
increased enhancement of active lesions with gadolinium.
Multi-infarct dementia → multiple hypo-dense areas without enhancement.
Toxoplasmosis, brain abscess, and lymphoma → Ring enhancing lesions seen on CT
scan
Cerebral atrophy → dilated ventricles with dilated sulci
Normal pressure hydrocephalus → dilated ventricles without dilated sulci. Patient is
“wet, wobbly, and weird.” (urinary incontinence, ataxia, and dementia triad is often seen
in these patients)
Alzheimer’s DiseaseBrain atrophy with or without periventricular white matter lesions
54 | P a g e
K N O W M E D G E
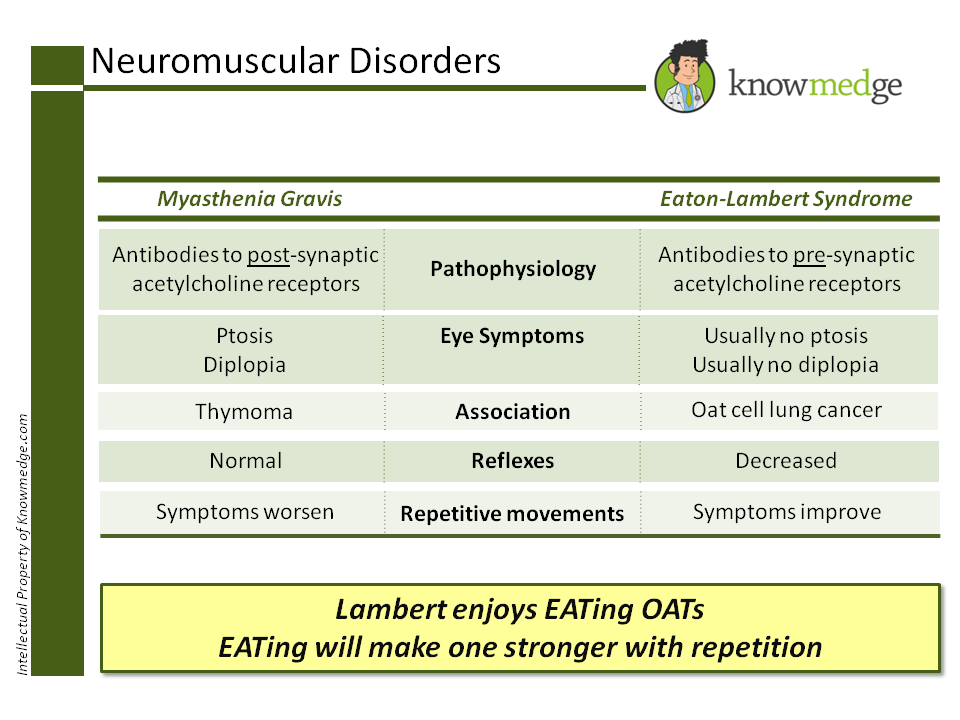
Pearl # 5: Differentiating Myasthenia Gravis and Eaton-Lambert Syndrome can seem
challenging at first. That’s why they’re on the ABIM.
Ever find yourself second-guessing whether it’s Eaton-Lambert or Myasthenia Gravis that
improves with repetitive movements? And, which one is associated with thymoma? Before
letting your head spin or do cartwheels, take a few minutes to learn the difference between
these two neuromuscular disorders. The concise yet useful categorization will make it difficult
to get the two mixed up.
Myasthenia gravis
Antibodies to post-synaptic acetylcholine receptors
Ptosis and diplopia can be presenting symptoms
Can be associated with thymoma
Reflexes are normal
Power decreases with repetition
Eaton-Lambert Syndrome
Antibodies to pre-synaptic acetylcholine receptors
Ptosis and diplopia are usually absent
Usually associated with oat cell carcinoma (small cell carcinoma) of the lung
Reflexes are decreased (hyporeflexia)
Power improves with repetition (“As you EAT, you get stronger”)
Let’s review it in Knowmedge slide form:
55 | P a g e
K N O W M E D G E
Once again, the folks who write the Internal Medicine med school clerkship shelf and ABIM
board exams don’t expect you to have the depth of knowledge regarding neurological
conditions that a neurologist possesses. However, topics such as the ones mentioned in the
slides and pearls above should assist you with the neurology section of these exams.
56 | P a g e
K N O W M E D G E
Quick and Easy Guide to Selecting the Right Topical Steroid
By: Dr. Sheila Krishna
Several of the most frequently utilized dermatologic treatments—especially for conditions that
arise in primary care and thus may be found on the dermatology portion of the Internal
Medicine board and medical school shelf exams—belong to the topical corticosteroid
category.
As there are dozens of options of various strengths, preparation, and container sizes (along
with the consideration of whether patients prefer generic vs. brand, over-the-counter vs.
prescription), it can be extremely overwhelming to select the “correct” topical corticosteroid.
Fortunately, in most instances, there is more than one reasonable treatment option that will
provide the patient with the relief they need.
Let’s begin by reviewing 5 Dermatologic pearls that will be helpful in your clinical practice and
may also help you select a couple more correct answers on the ABIM board exam.
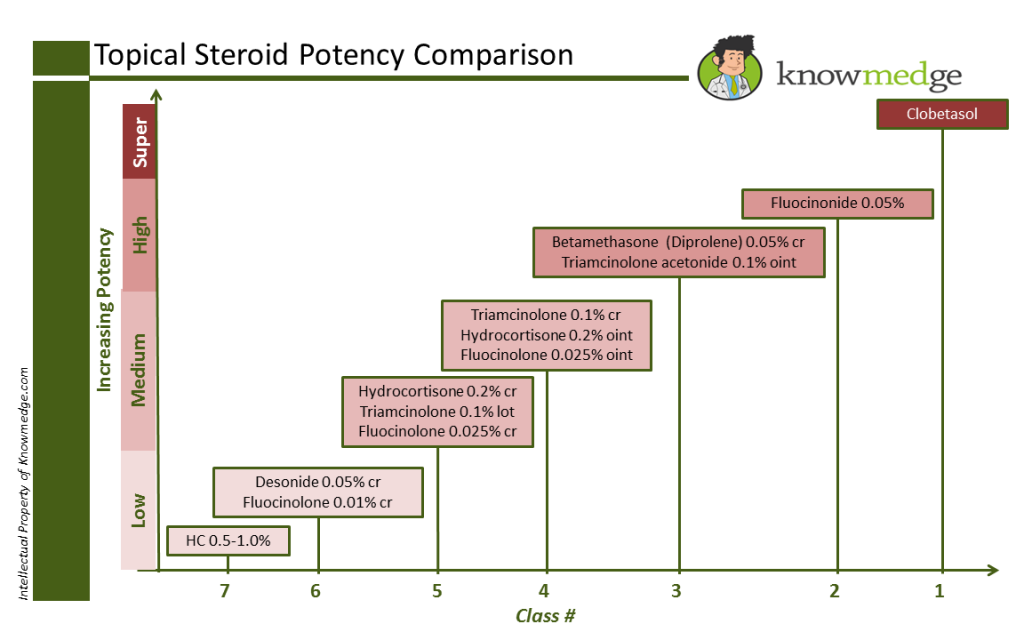
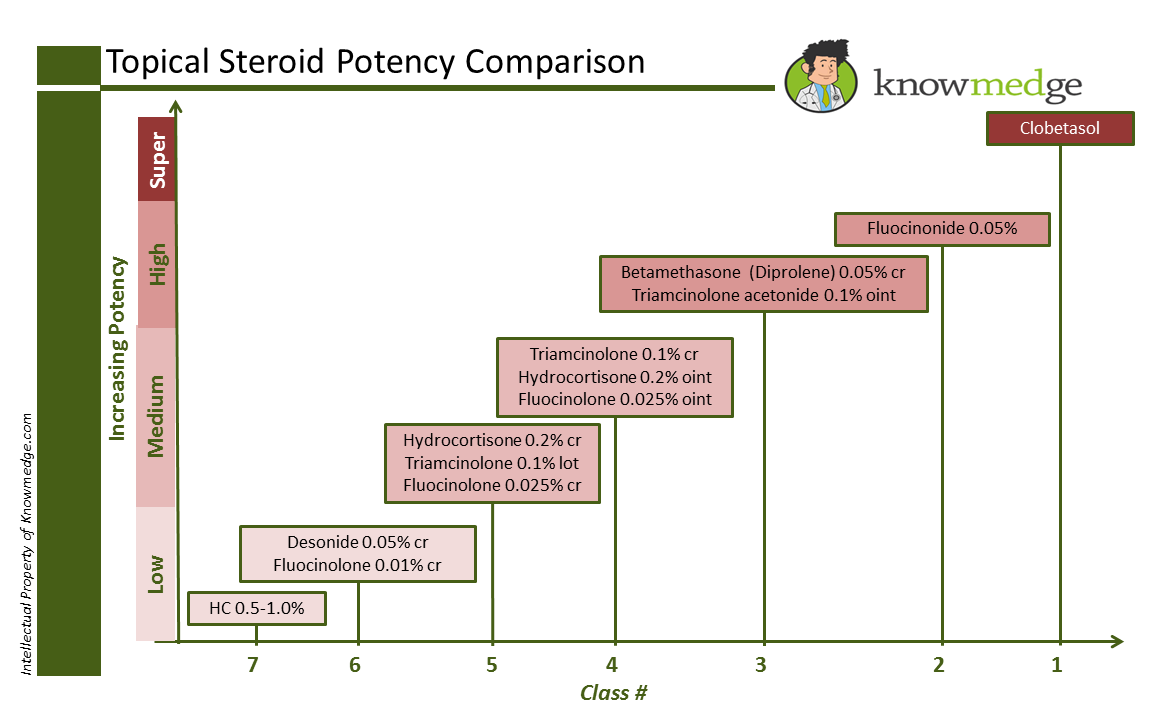
Pearl # 1: Know the different strengths of the topical corticosteroids.
There are a total of 7 different classes of topical corticosteroids, with class 1 representing the
highest potency and class 7 representing the lowest potency. It’s critical to be able to
recognize the medication’s potency because we need to find the best match for the patient’s
condition—strong enough to treat the disease but gentle enough to avoid unnecessary side
effects. In Knowmedge fashion, here’s a slide that gives the most commonly used topical
corticosteroids with their class number and relative potency.
57 | P a g e
K N O W M E D G E
Class 1 and 2 topical corticosteroids should never be prescribed on the face of body folds or
groin as these areas have more fragile skin that can be damaged by the skin-thinning potential
of these stronger topical agents.
Pearl # 2: When pressed for time, consider these selections.
For treating non-folded trunk and extremities, Triamcinolone 0.1% is a good option. For
treating the face and body folds (e.g. axilla, groin, inframammary areas, panniculus), Desonide
or Hydrocortisone can be used. For the palms and soles, Fluocinolone or Clobetasol may be
tried.
Pearl # 3: Select the correct preparation
58 | P a g e
K N O W M E D G E
Once you think you have the right medication selected, you may pause when asked by your
electronic prescription-ordering system or your local pharmacist which preparation you are
ordering: cream, ointment, or lotion. Make sure that the patient has been consulted about their
preferred preparation since they may not be adherent with the treatment plan if they find it
makes them feel uncomfortable.
From a cosmetic acceptance standpoint, creams tend to be an acceptable option since they
absorb well and lack the greasy texture of ointments. However, keep in mind that they may
sting if applied to open areas of the skin and they can contain preservatives that can lead to
an allergic contact dermatitis.
Ointments usually contain petrolatum, which provides more of an emollient effect to help retain
water. They are less likely to sting than creams. The biggest issue is the greasy texture that
some patients find uncomfortable. Lotions are more water-based than oil-based. As a result,
they are easily absorbed into the skin and spread easily, making them a good choice for
covering large areas of the body.
Pearl # 4: Finding the correct amount to prescribe
Unlike the straight-forward exercise of selecting the quantity of oral medications—90 days of
a once daily medication equals 90 pills—providing enough topical agent to last a patient until
the next scheduled refill is a bit more challenging. If too little is prescribed, they will be
frustrated by frequent trips to the pharmacy, not to mention the high co-pay they may be
dishing out each time they visit.
A good rule of thumb to use is that 1 palm is 1% of the body when estimating the % of the skin
that is affected by the patient’s dermatologic condition. Most topical corticosteroids come in
30 to 60 gram tubes. For a typical 70-kg patient, a 30gram tube provides one application to
the entire body.
59 | P a g e
K N O W M E D G E
Pearl #5: Don’t forget the importance of gentle skin care
Atopic dermatitis and xerosis may not resolve despite topical corticosteroids if patients
continue to add agents to their skin which can increase drying. Harsh body washes and soap
and laundry detergents can do a number on the skin. Tell patients to avoid those and instead
apply emollients, which consist of water-supplying moisturizers (e.g. coconut oil, mineral oil)
and water loss-reducing occlusives (e.g. petroleum jelly).
60 | P a g e
K N O W M E D G E
8 Pulmonary Disease & Critical Care Pearls
By: Dr. Sunir Kumar
Pulmonary disease and critical care are an extremely important part of the Internal Medicine
Medical Clerkship and ABIM Board exam. According to the ABIM exam blueprint, questions
testing pulmonary disease topics comprises ~10% of the exam. That places it second only to
cardiology’s 14% in terms of relative percentage.
Pearl # 1: ABGs do not need to stand for AnyBody’s Guess
The next time you see an arterial blood gas (ABG) on a practice or actual exam question,
don’t start searching for the “Panic” (or “Skip”) button. Determining diagnoses based on ABGs
can seem daunting at first but by following a simple yet systematic approach, we can tackle
these questions without difficulty. Click on the link to our previous “How to Handle ABGs on
the ABIM Board Exam” and after reviewing the 5 easy steps, it won’t be long before you look forward to ABG questions on the exam.
Pearl # 2: Obstructive or Restrictive? That is the question surrounding Lung Disease
To distinguish between obstructive and restrictive lung disease, the first value to look at on
the pulmonary function test (PFT) report is the Total Lung Capacity (TLC), which is defined as
the volume of air contained in the lungs at the end of a maximal inspiration.
Obstructive Lung Disease: TLC will be increased (example: asthma and COPD)
Restrictive Lung Disease: TLC will be decreased. Restrictive Lung Disease is further
sub-divided into intra-thoracic and extra-thoracic lung disease.
o Intra-thoracic lung Disease (FEV1/FVC normal or increased above 80%, DLCO
decreased, Residual Volume decreased)
Sarcoidosis
Idiopathic Pulmonary Fibrosis
Hypersensitivity Pneumonitis
Pneumoconiosis
ABPA
Churg-Strauss Syndrome
Asbestosis
61 | P a g e
K N O W M E D G E
Silicosis
Berylliosis
o Extra-thoracic Lung Disease (FEV1/FVC normal or increased above 80%,
DLCO normal, Residual Volume increased)
Obesity
Kyphosis
Myasthenia Gravis
Guillain-Barre Syndrome
Muscular dystrophy
Pearl # 3: The Mnemonic “CHAD PARS” helps recall the major causes of
{kind=link}