By: Dr. Sunir Kumar
Oncology is an essential part of the Internal Medicine Medical Clerkship and ABIM Board
exam. According to the ABIM exam blueprint, questions testing Oncology topics comprise
~7% of the exam. Initially, oncology seems like a very difficult subject given how the treatment
regimens of the many types of carcinomas are ever-changing. However, realize that Internal
Medicine exams are focused on the basics of the different malignancies. These 8 pearls will
get you off to a good start for identifying
Pearl # 1: Which cancers correspond to lytic bone lesions? Blastic? Lytic or Blastic?
Lytic bone lesions
o Melanoma
o Multiple Myeloma
o Renal cell cancer
o Thyroid cancer
Blastic bone lesions
o Prostate cancer
Lytic or blastic lesion
o Lung cancer
o Breast cancer
45 | P a g e
K N O W M E D G E
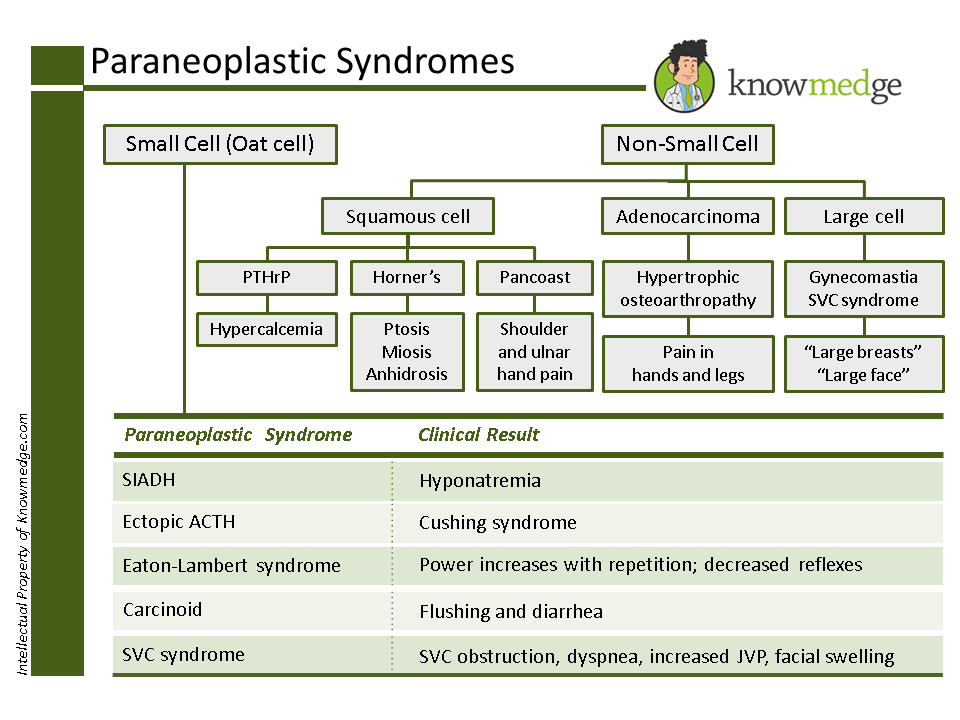
Pearl # 2: Which paraneoplastic syndrome goes with which cancer?
Pearl # 3: Know these high-yield Breast Cancer facts for the ABIM and IM shelf exams
If the lesion is >1cm OR the patient has lymph node involvement → chemotherapy will
be part of the treatment protocol.
If sentinel node biopsy is negative → no further lymph node biopsy is required
If the patient’s breast cancer is ER/PR (+) and patient is pre-menopausal →Tamoxifen
is given for 5 years
If the patient’s breast cancer is ER/PR (+) and is post-menopausal → Aromatase
inhibitors (eg. Anastrozole) is given
If the patient’s breast cancer is HER2/neu (+)→ Trastuzumab is given →can cause
CHF →check echocardiogram to assess left ventricular function
46 | P a g e
K N O W M E D G E
Triple negative breast cancer (ER negative, PR negative, HER2/neu negative) has the
worst prognosis
Pearl # 4: Don’t let chromosomal translocations overwhelm you
t (14,18) → Follicular Lymphoma
t (8,14) → Burkitt’s Lymphoma
t (9,22) → Known as Philadelphia Chromosome (BCR-ABL) gene fusion → good
prognosis in CML patients and bad prognosis in ALL patients
t (15,17) → Acute promyelogenous Leukemia (M3) → good prognosis → Treatment is
with All-Trans Retinoic Acid (ATRA)
t (11,14) →Mantle cell Lymphoma → highly aggressive form of Non-Hodgkin’s
Lymphoma → cyclin D1 oncogene is overexpressed → treat with R-CHOP
47 | P a g e
K N O W M E D G E
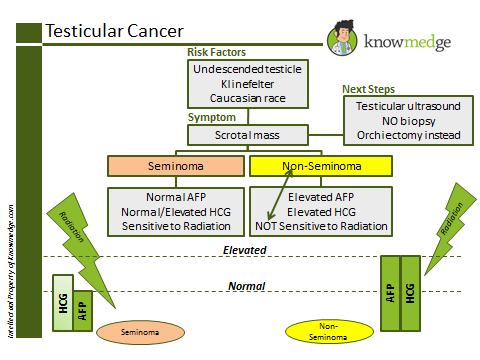
Pearl # 5: Testicular cancer is broken down into seminomas and non-seminomas
Seminomas are Radiation sensitive and usually have a normal AFP and HCG level
(although HCG can be elevated in 5-10% of cases)
Non-Seminomas (e.g., yolk sac tumor, embryonal carcinoma, teratoma,
choriocarcinoma) are radiation resistant and usually have elevated AFP and HCG level
Pearl # 6: High-yield facts about Colon Cancer for the ABIM and IM Shelf Exam
If cancer invades mucosa or sub-mucosa → colon resection is required
If cancer invades muscularis propria, serosa, or has LN involvement →colon resection
is required +chemotherapy (usually FOLFOX) +/- Irinotecan. FOLFOX is 5 Flurouracil,
Oxaliplatin, and Leucovorin
Most common area of metastasis for colon cancer is the liver
If solitary liver lesion →resection of liver can be performed
If multiple liver lesions → poor prognosis and survival rate is low
Pearl # 7: Must know Oncological Emergencies
48 | P a g e
K N O W M E D G E
Superior Vena Cava Syndrome → caused by obstruction to the superior vena cava
leading to:
o Neck and facial swelling
o Dyspnea
o Cough
o Physical examination will show distended jugular veins
o Chest x-ray may reveal mediastinal widening or right hilar mas
o Most common cause is lung cancer (particularly small cell lung cancer).
Malignant lymphoma is also a well-known cause of superior vena cava
syndrome
o Management obviously requires treatment of the underlying malignancy but
symptomatic measures such as diuretics and elevation of the bed usually suffice
Spinal cord compression
o Most common cancers that cause spinal cord compression are: lung cancer,
breast cancer, prostate cancer, multiple myeloma, and lymphoma
o Back pain is the most commonly presenting symptom. Other concerning
symptoms include muscle weakness, numbness/tingling, cauda equina
syndrome, and loss of bowel or bladder control
o Diagnosis is required promptly to prevent further neurological deterioration and
an MRI of the entire spine should be ordered
o Management for spinal cord compression is with Dexamethasone 10 mg IV X 1
dose, followed by Dexamethasone 4 mg IV every 6 hours
o Radiation therapy can help in shrinking the tumor; however, recent studies
indicate that surgical decompression is superior to RT. Therefore, an immediate
neurosurgical consultation is required when this condition is suspected or
diagnosed
Tumor Lysis Syndrome
o Intracellular contents leak out into the bloodstream
o Although this condition can occur with any malignancy, it is more common in
aggressive lymphomas and hematological malignancies
o Hyperkalemia, Hyperuricemia, Hyperphosphatemia, Acute renal failure, and
Hypocalcemia are often seen in patients with tumor lysis syndrome
49 | P a g e
K N O W M E D G E
o Management of tumor lysis syndrome requires electrolyte abnormality
correction, aggressive hydration, and allopurinol
Once again, the folks who write the Internal Medicine licensing exams don’t expect you to have
the depth of knowledge regarding the plethora of cancer diagnoses that an oncologist possesses.
However, topics such as the ones mentioned in the pearls above should assist you with the
oncology section of the med school clerkship shelf and ABIM board exams.
50 | P a g e
K N O W M E D G E