The extract below from ‘A Bridge Too Far’ was published on the free e-books site on October 16, 2012. The book has been downloaded 3,200 times since publication.
|
|
‘Late April 2004, whilst employed by Deloitte & Touch subsidiary Commercial & Industrial Computer Services, my schedule entailed attending an important meeting called by the councillors at the Ilembe District Municipality on the North Coast of Natal, then travelling south by car all the way down that Coast and inland to the municipality at Kokstad. After a number of meetings there, in a stay over of three days, I travelled North East across the Little Drakensburg Mountains to the municipality at Howick then motored back on the N3 Highway to Johannesburg. The following day on the way to work with Diane in the car, I experienced a sharp pain in my right temple which caused me to swerve off the road and stall the vehicle. I would later find out through medical experts that I had suffered a Transient Ischemic Attack. |
I was examined on April 17 by a well-known neurologist, Dr van Heerden, who was not too concerned by the incident and never once considered that I had suffered a
|
|
Transient Ischemic Attack. He did however order a CT scan to be carried out on May 6, 2004. On examining the scans Dr van Heerden gave me a clean bill of health despite the radiologist not agreeing with him. On May 10 the good physician happily departed for his annual ski trip to the Swiss Alpine region. On the Sunday morning of May 30, 2004, while serving coffee to Diane in bed, I suffered a massive internal cerebral haemorrhage. On that day I was treated by paramedics at home and stabilised before being taken by ambulance to the Intensive Care Unit at the Olivedale Clinic in Johannesburg North. On admission I was diagnosed as having had an intra-cerebral haemorrhage with complications of Type 11 Diabetes, Hypertension and Hyperlipidaemia. Clinical evaluation was Left Hemiparesis, Mild Expressive Aphasia and Full Continence. |
The wrinkled grey haired fellow with lederhosen had just cooked his goose’.
|
|
My current state of ill health and immobility thirteen years later are a direct consequence of the degenerating effects of the stroke and poor management of diabetes. The haemorrhage had occurred on the right-hand side of my brain. Strokes usually affect only one side of the brain. Movement and sensation for one side of the body is controlled by the opposite side of the brain. |
The left-hand side of my body was thus adversely affected.
STROKE TRAUMAThe right side of the brain controls the ability to pay attention, recognize things you see, hear or touch, and be aware of your own body.
In most people, the left side of the brain controls the ability to speak and understand language.
A haemorrhage in the right side of the brain usually causes the following problems:
Neglect
You may ignore the left side of your body or your environment. This means you may not turn to look toward your left side or you may not recognize things that are on your left.
PerseverationYou may have difficulty following instructions or answering many questions asked one right after the other. You may repeat answers or movement even though a new instruction was given or a new question asked.
Visual and spatial problemsYou may have problems judging distance, size, position and rate of movement and how parts relate to a whole.
Source: Allina Patient Education, Understanding Stroke: Information about Stroke and Recovery, fourth edition, ISBN 1-931876-13-4.
What is not indicated in the above article is that when the carotid artery is severed from the brain after a stroke, the blood is pumped unfettered into the brain cavity. As a result blood does not reach the nerve endings until the blood supply is continued to the brain.
The length of time between the rupture and repair of this artery is critical to the amount of damage inflicted on the nerve endings. Once the nerve endings die through lack of blood, they cannot be repaired nor regrow. The damage results in perpetual ‘pins and needles’ in the affected areas of the body.
Human beings distinguished themselves as bipeds through the evolution of four senses which allowed them the eventually stand upright.
Apologies for the pigeon medical explanation above but it did originally come from some or other physician and has been mangled by this dumb accountant.
The upshot, however, is that the irreparable damage to the nerve endings in a right sided stroke causes permanent balance and tactile problems in the left-hand side of the body.
EMOTIONAL LABILITYAnother peculiar condition resulting from a stroke is emotional lability.
What is emotional lability?
Emotional lability refers to rapid, often exaggerated changes in mood, where strong emotions or feelings (uncontrollable laughing or crying, or heightened irritability or temper) occur. These very strong emotions are sometimes expressed in a way that is not related to the person’s emotional state.
What causes emotional lability?
Emotional lability occurs because of damage to parts of the brain that control:
When a person is emotionally labile emotions can be out of proportion to the situation or environment the person is in. For example, a person may cry, even when they are not unhappy – they may cry just in response to strong emotions or feelings, or it may happen “out of the blue” without warning.
A person may have little control over the expression of these strong emotions, and they may not be connected to any specific event or person.
Following brain injury an individual may also lose emotional awareness and sensitivity to their own and other’s emotions, and therefore their capacity to control their emotional behaviour may also be reduced. They may overreact to people or events around them – conversations about particular topics, sad or funny movies or stories. Weaker emotional control and lower frustration tolerance, particularly with fatigue and stress can also result in more extreme changes in emotional responses.
This is why I cannot watch Little House on the Prairie.
DIABETESAs regards the diagnosed diabetes a different set of challenges arose. The excess blood sugar in diabetes can wreak havoc on blood vessels all over the body and cause complications. It can severely damage the eyes, kidneys, nerves, and other body parts; cause sexual problems; and double the risk of heart attack and stroke. Some people with type 2 diabetes need insulin, but most don't.
Hyperglycemia (high blood sugar) may be the hallmark of diabetes, but does not cause most of the morbidity (the harm of the disease). Blood glucose is fairly easily controlled by medication, but this does not prevent the long-term complications. Despite blood glucose control, damage occurs to virtually every organ system.
It would be difficult to find a single organ system not affected by diabetes. These complications are generally classified as either microvascular (small blood vessels) or macrovascular (large blood vessels).
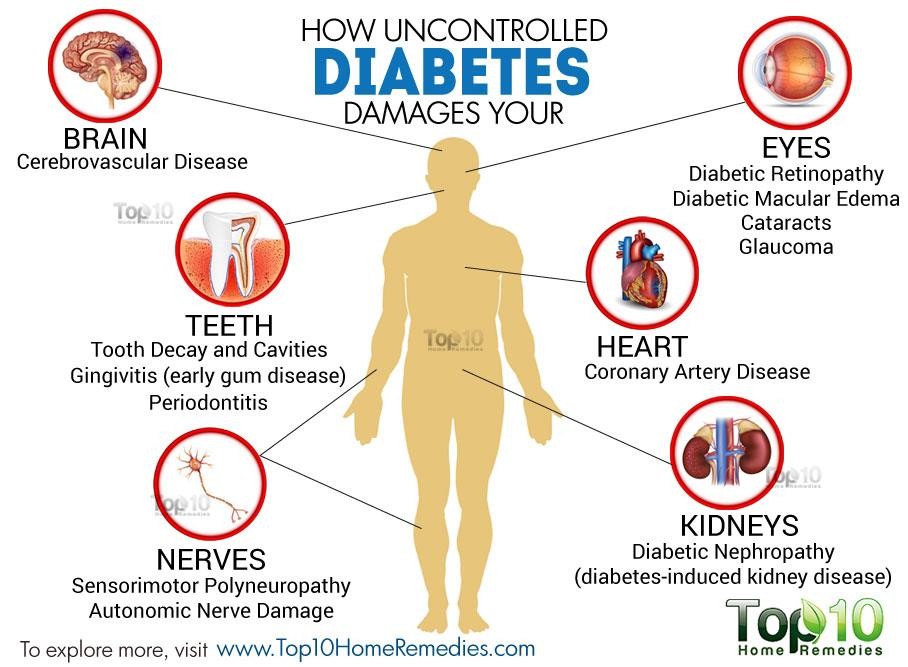
Certain organs, such as the eyes, kidneys and nerves are predominantly perfused by small blood vessels. Chronic damage to these small blood vessels causes failure of these organs. Damage to larger blood vessels results in narrowing called atherosclerotic plaque. When this plaque ruptures, it triggers an inflammatory reaction and blood clots that cause heart attacks and strokes. When blood flow is impaired to the legs, it may cause gangrene due to reduced circulation.
There are other complications do not fall neatly into this simple categorization. A variety of diabetic complications are not obviously caused by injured blood vessels. These would include skin conditions, fatty liver disease, infections, polycystic ovarian syndromes, Alzheimer’s disease and cancer.
To continue from ‘a Bridge Too Far….
‘Based on the aforementioned medical diagnosis I was ordered to give up smoking, undergo intense rehabilitation, subscribe to a very strict diet, refrain from alcohol, consume prescribed chronic medication daily and work for only two hours a day.
Under these conditions I was given a fifty percent chance of survival by the physicians.
My first concern was for Diane. Her family support base was back in KwaZulu Natal and, if I did not make it through this crisis, she would be left alone in Gauteng without meaningful financial support. So, in a whirl of activity, we got married in hospital. This ensured that if I died, Diane, as my dependent, would receive the proceeds of an insurance policy taken out on my life by Deloittes when I had joined the company. The hospital was amazing. Besides paying for the event, they made many of the last minute and rushed arrangements including inviting patients of the hospital as guests to the ceremony.
Marry they did but die he did not.
|
|
After ten days I was considered by Specialist Physicians de la Cour and Teuwen to be stable enough to be moved from High Care at Olivedale to the Netcare Rehabilitation Clinic in Aukland Park. There I underwent thirteen days of intensive rehabilitation including: dietary and cholesterol advice, physiotherapy, occupational therapy and also neuro psychology treatment. Against all advice by attending doctors, psychologists and physicians, the treatment was terminated by the Fedhealth Medical Aid Scheme on June 23, 2004. |
Rehabilitation unassisted at home was totally inadequate and, following a lengthy tussle with Fedhealth, I was allowed again to continue treatment at Netcare Clinic in Aukland
|
Park. The disrespectful and disgraceful length of time that it took for Fedhealth to agree to further rehabilitation ensured that I would not be recommending their services anytime soon. In negotiating the additional rehabilitation with Fedhealth, transport became a stumbling block. The cost of an ambulance, upon |
|
which Fedhealth insisted, proved to be too exorbitant. You will know that an ambulance ride today costs just a little less than a seat on the space shuttle. So I independently negotiated a rate from an under-utilised VIP Limousine Service Company. They were happy to offer their idle personnel and vehicles for hire during the day. Thus for the entire duration of my rehabilitation I was ferried to and from the Aukland Park Rehabilitation Facility in a shiny black stretch limousine driven by a
pistol toting ex wrestler in a dark suit, wearing sunglasses and bearing a sinister and menacing demeanour.
Our arrival and departure from the Rehabilitation Clinic was the subject of much speculation by patients and staff alike. It was a complete mystery to them who this persona, guarded by the Mafia and arriving in a black stretch limousine might be. I am embarrassed to admit that I added to the drama by always wearing shades and carrying my kit in a suspicious black suitcase.
Between October and December 2004 I duly underwent further intensive rehabilitation including speech therapy, psychological treatment, physical conditioning, physiotherapy and occupational therapy. In addition, I resumed my daily ten kilometre walking and swimming regime in my own time. All of this intense rehabilitation started to deliver results.
By December 2004, the chart recording my progress under this regime had improved from 15/60 to 45/60. Real progress!
I recommenced work duties again in January 2005, albeit doing only mundane office routines. In the ensuing four months it became obvious that I would sadly be unable to return to my former Account Executive responsibilities. By April 2005 my chart reflected a regression back to 21/60 from 45/60. I was almost as bad as I had been the previous October.
Under these circumstances the managers, doctors and insurers had no other option but to regard me as permanently disabled and I was duly boarded.
It was a lonely existence for a while as Diane was away on trips to far flung municipalities most weeks and I was left kicking my heels at home. Deloittes helped by allowing me to tag along, for example, when Diane trained people at Ilembe on Kwa Zulu’s North Coast.
When Diane got retrenched a few months later, there was no longer any compelling
|
reason to remain in Johannesburg and we therefore made our arrangements move back to Durban and its glorious beach front……..we were headed home again. A testimonial from Alan Yorke, the Partner at Deloitte & Touche, based then in Pretoria, reads: “Bryan Britton was employed by Deloitte CICS and |
|
was employed as an Account Executive responsible for sale and implementation of the Munsoft Software System developed specifically for Local Government in South Africa. Bryan has also attended training courses hosted by Deloittes on GAMAP and
was able to identify some of the more difficult areas of GAMAP that impact on municipalities in South Africa. Bryan is moving back to Durban and may be in a position to assist Deloittes there on municipal accounting assignments.
On May1, 2005 I was placed on full disability pension by the Employee Benefit Division of Sage Life Limited. Sage would later be taken over by the larger Momentum Life Group, who remains my employer to this day.
The conditions of my disability benefit are that I do not leave South Africa and do not earn any other form of income. My medical and psychological prognosis has determined that I should observe a strict cholesterol free diet devised for diabetics, avoid alcohol and read or work no more than two hours a day.
I am required to have a medical examination every three months and then, once a year, attend a Momentum essential review process. This accompanies an annual application to Momentum to continue on the disability benefit for the following year.
If the annual application succeeds, then an increase of no more than five per cent applies for the ensuing year's benefits. I have to ingest a daily dosage of:
Simvastatin Enalapril
Indapamide Ecotrin
Amplodipine Diamicron
Atenolol Glucophage
The effects of the stroke are irreversible and I am left with no feeling in the foot, leg, arm and hand on my left side. This results in impaired balance and rules out speed walking, swimming and strenuous exercise. As a result I am obliged to watch my diet
|
extremely closely. The effects are also unfortunately degenerative and have necessitated giving up driving. I believe that I could present a danger to other motorists should the stroke reoccur while driving. So I unfortunately had to ditch the fancy wheels. Over time the conditions will worsen. My disposition and faith, however, remain upbeat and unshakable. I am not unhappy with the cards that the Lord has dealt me this time. For many years in the past I |
|
have been dealt hands with which I have been able to stay productively at the gaming table of life. And I have won more than a few hands over time. For this reason I have no real complaints and have no regrets. In fact, I have been blessed in my life with a still active mother, a brother whom I love, two wonderful marriage partners, three magnificent sons whom I love dearly, seven healthy and intelligent grandsons and one adorable granddaughter, two incredibly smart stepsoand an absolutely gorgeous stepdaughter. It doesn't get much better than that.
Although Diane and I agreed to divorce in 2011, we remain close friends and see each other regularly. Being younger and fitter than I am, it is only fair that she be free to enjoy the rest of her life without being burdened by my afflictions. I pray that she finds lasting love, good health, peace and fulfilment in the remaining years of her life’.